Flu Shot
MOH gives free influenza vaccination to it's staffs. Those who haven't get theirs can check with your hospital pharmacy or sister in-charge of your ward.
I found a letter from our pharmacy in the file unattended last few weeks ago and asked our ICU sister to contact our hospital pharmacy. In bolehland, almost nobody will going to give u anything (even if it is their job to do so) if we dun ask for it.
Received my flu shot (
Fluarix) for 2006/2007 last week. It is an inactivated influenza vaccine contains:
A/New Caledonia/20/99 (H1 N1 )-like strain:
A/New Caledonia/20/99 (IVR-116),
A/Wisconsin/67/2005 (H3 N2 )-like strain: A/Wisconsin/67/2005 (NYMCX-161),
B/Malaysia/2506/2004 – like strain: B/Malaysia/2506/2004.
Medscape has an interview report on this:
Influenza Vaccination and Healthcare Workers: An Expert Interview With Kristin Nichol, MD, MPH, MBAIt was reported by CDC that vaccination levels for healthcare workers are typically less than 40% (and this is in kia-su ama-rica, think what would our figgure show?)
Dr. Nichol: I advocate very active and vigorous influenza vaccination programs within the healthcare setting for healthcare workers.
Seroprotection is generally obtained within 2 to 3 weeks. Flu season can start as early as Oct and end as late as May.
CDC has this to say about who should get the shot:
People at high risk for complications from the flu, including:
Children aged 6 months until their 5th birthday,
Pregnant women,
People 50 years of age and older, and
People of any age with certain chronic medical conditions;
People who live in nursing homes and other long term care facilities.
People who live with or care for those at high risk for complications from flu, including:
Household contacts of persons at high risk for complications from the flu (see above)
Household contacts and out of home caregivers of children less than 6 months of age (these children are too young to be vaccinated)
Healthcare workers.
There are still a lot of us (health care workers) don't want to get the shot for all sorts of reason...
Among people who were not immunized, we saw a variety of reasons, including unfamiliarity with the national recommendations, misperceptions about why they are in a target group [for vaccination], and misperceptions about the safety and effectiveness of vaccination.
Here's the definition of healthcare provider included in the ACIP and the Healthcare Infection Control Practices Advisory Committee (HICPAC) statement, published in February 2006:
A healthcare provider refers to all paid and unpaid persons working in healthcare settings who have the potential for exposure to infectious materials, including contaminated medical supplies. Healthcare providers might include but are not limited to: physicians, nurses, nursing assistants, therapists, technicians, emergency medical service personnel, dental personnel, pharmacists, laboratory personnel, autopsy personnel, students and trainees, contractual staff and persons, for example, clerical, dietary, housekeeping, maintenance and volunteers not directly involved in patient care but potentially exposed to infectious agents that can be transmitted to and from the healthcare provider.
So do u want to get ur shot?
Traditional/ Complementary Medicine in Public Hospital
Recently MOH called for a meeting in Hospital Kepala Batas (the integrated hospital in the north) to shed more light to us regarding the MOH's vision and it's plan of rolling out T/CM service in public hospital.
Coincidentally,
Bernard and
Malaysia Medical Resources blog about this issue too.
MOH is really serious about integrate T/CM into public hospital system and they really want it to work.
RMK-9 (Rancangan Malaysia ke-9) will see 3 hospitals (Kepala Batas, Putrajaya and Sultan Ismail) to run the pilot project starting June 2008. It would starts with out patient T/CM clinic. They paln to extend this service to all state GHs in RMK-10.
At this moment, MOH is still drafting the guidelines and a new TCM Bill. So we don’t know in detail what it would be yet (sounds like PHFSA?).The
TCM Division of MOH promises there well tight monitoring with new bill and guidelines to guide this services. There will be many roadshows in the future to brief MOH’s staffs regarding this TCM practice in MOH hospitals.
The services include Acupuncture, Herbs in oncology and Malay Massage (was told that DG has special interest in this and wants more ‘research’ to be carry out on this) and some others like homeopathy, aryuvedic etc. The scary one include aroma therapy!
According to pengarah of bahagian TCM, it would be a walk-in out patient setting for the starter. They might draft changes in the Medical Act 1971 to enable doctors to refer cases to TCM.
The TCM Act/Bill is suppose to be out in mid Dec 2006. This would include APC, TCM council, TCM Professional Body, Qualifying examination to practice (for those old shinseh without diploma or degree), insurance etc.
The guidelines are suppose to be very comprehensive, which include list of dos n don’ts, what they can treat, standard protocols etc. I hope they consult enough ppls and make a RIGHT guidelines.
It is said that the TCM practitional cannot issue MC but they can recommend one. So i can predict there will be many patients from TCM clinic come lining up in the Casualty (A&E) of Hospital Kepala Batas to get a MC from the poor MO on duty there. So can the MO just gave the MC as per recommedation of TCM practitional without examine the patient? No? Then he/she has to see the patient all over again?
What about medical reports? Or can the TCM practitional order x-ray, CT scan, blood test etc?? I hope all these issues are addressed in the coming guidelines.
The T/CM practitioners cannot use DR in their name, but hear this, those with degree will be in Gred 41-54 like doctors in govt service (But I dun think they will be in category 'U'). Those with diplomas will be in gred 29-38 like our nurses and MAs.
Works are already being done to regconise TCM degrees from 3 universities in China (Beijing, Shanghai and ?Nanjing).
The enforcement unit of MOH TCM Division, will be up and running latest early next year. They will be incharge of monitoring etc… It wouldn't be difficult to monitor 3 out patient clinics in the pilot phase. How efficient are they in monitoring n enforcing laws in RMK-10 when all state hospitals will have TCM service?
More on AACA2006
Who is this gentleman?

He is Prof Ronald D Miller, the towering man in anaesthesia. I'm sure everybody who r in anaesthesia knows him but probably dun regconise him.
He delivered the 1st plenary talk about the future of anaesthesiology in the 12th AACA. The photo below is an endoscopic appendisectomy done by a robot. There is no surgeon and scrub nurses in the OT except the anaesthetist.
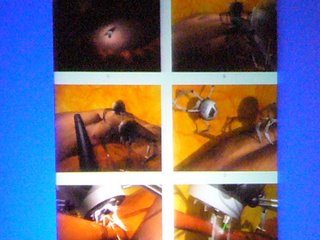
There are already prototypes of anaesthesia machines that can monitor the parient remotely and gives all range of anaesthesia related drugs automatically in response to patients need. Prof Miller was saying that in 20 years to come, anaesthetist is not required in OT anymore!
Guess we are going to be out of job eh? He was really believed that technology will change the way we work. The are machine can intubate the most difficult intubation, canulate the most difficult vascular access... ect etc.
Not untill a man from india stood up and told him that in India, although the have very good center comparable to american standard, but vast majority of the country still lagged behind with only the very basic setup. We are talking about GA without SpO2 monitoring, no ETCO2 monitoring and no ventilator machine but hand bagging the whole operation etc etc...
There will be more divide on countries with money to buy new technologies and countries that cannot....
In Malaysia, I'm sure we won't be out of the job yet at least for another 40 years.
Challenges in PAIN Management. This is a seminar on chronic pain organise by Hospital Ipoh and
Malaysia Association for the Study of Pain (MASP) which will be held on 8th-10th Dec 2006 in Hospital Ipoh.
Click on this
link to download the registration form. Closing is on 28/Nov.
If I get some locum in the next 2 weeks to cover the rm200 registration and the extra for accomodation, I'll see u guys there too. :)
AACA 2006 - The Art & Science of Anaesthesialogy

Just came back from the 12th Asian Australasian Congress of Anaesthesiologists, Singapore.
Presented a poster at the conference and the '
kembang moment' was when the editor-in-cheif of
Acute Pain invited us to publish the paper in his Journal. Well, it is not a high impact journal like
Aesthesia & Analgesia,
Anaesthesiology,
BJA and
Anaesthesia etc because it is only 2nd year in publication. Our own Prof Ramani from UM is one of the associate editor.
I'd think that's the best I get out of this trip to Singapore. On the other hand,
SGH is all out to recruit too. They have a booth for recruitment at the congress venu. (No, I didn't plan to leave Malaysia, not yet).
Also met and spoken to Prof Chan, Prof Ramani and A/Prof Lee CY at the conference.




